Antacids analysis
ICP,
![]() 2 Min
2 Min
This site is intended for Healthcare Professionals only
ICP,
![]() 2 Min
2 Min
ICP,
![]() 2 Min
2 Min
Indigestion and dyspepsia are terms used to describe a range of vague symptoms in the upper gastrointestinal tract associated with the ingestion of food.
There are several possible causes, but moderately raising stomach pH generally relieves symptoms. OTC treatment is therefore aimed at either neutralising gastric acid or suppressing its secretion, with:
• Antacids
• Ranitidine, an H2-antagonist
• Proton pump inhibitors.
This article will deal with the first of these treatments and associated constituents, the other two will be covered next month.
 ANTACIDS
ANTACIDSHow do they act?
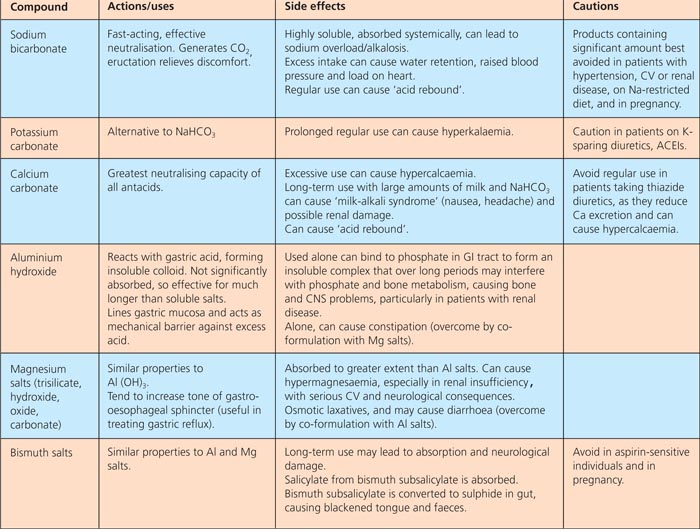
Several alkali metal salts are used in the treatment of indigestion. They are weak bases which dissociate to form alkaline salts, thereby neutralising gastric acid. Antacids used in indigestion treatments have different neutralising capacities, and the degree to which they are absorbed systemically also varies, influencing their duration of action. Soluble salts act quickly but are absorbed rapidly, reducing their duration of action. Salts of divalent and trivalent metal ions are insoluble and have a less rapid but more prolonged action. Antacid medicines are generally combinations of two or more compounds, with the aim of producing a formulation that is fast acting, with a high neutralising capacity, which is not absorbed into the body and with a long duration of action.
The properties of antacid compounds are summarised in the table.
Interactions
• Antacids can interfere with the absorption of many drugs, including: tetracyclines, quinolone antibacterials and penicillamine, to form insoluble metal ion chelates.
• Absorption of tetracyclines, ketoconazole and itraconazole is reduced in the presence of antacids, as they are less readily soluble in an alkaline than an acid medium. Absorption of azithromycin, nitrofurantoin, rifampicin, phenytoin, chloroquine, phenothiazines and bisphosphonates is also likely to be reduced.
• The action of enteric-coated drugs, formulated to resist gastric acid and dissolve in the more alkaline medium of the duodenum, may be disrupted, causing unwanted release of drug in the stomach.
• As antacids can interfere with the absorption of so many drugs, patients are best advised to leave an interval of at least two hours between taking a dose and any other medicine. And it has been shown that antacids exert the most prolonged effect when taken one hour after meals.
• Antacid preparations containing sodium bicarbonate should be avoided by patients on lithium therapy as sodium ions are preferentially reabsorbed in the kidney, increasing lithium excretion and reducing plasma lithium concentrations.
Alginates
Alginates act as reflux suppressants. They precipitate out in the acidic medium of the stomach to form a sponge-like polymer matrix of alginic acid which fills with carbon dioxide bubbles, generated by the reaction between stomach acid and sodium or potassium bicarbonate included in alginate-containing preparations, forming a raft that floats on top of the stomach contents. When peristalsis occurs, stomach contents are pushed up against the diaphragm and the alginate raft, which is forced towards the gastro-oesophageal junction, forms a physical barrier against the reflux of stomach contents into the oesophagus.
Antiflatulent: simeticone
Distension of the stomach caused by trapped gas often contributes to the discomfort of indigestion. Simeticone is a silicone-derivative surface-active agent included in some antacid products and also available on its own as tablets or capsules. Its surfactant activity helps to coalesce small gas bubbles into larger ones, which are then vented by eructation.
• Antacids have been used for many generations and their continuing popularity seems to attest to patients’ satisfaction with them. But there is little published evidence of their efficacy and nothing recent. The Cochrane Library is undertaking a review of pharmacological interventions for non- ulcer dyspepsia and a previous version has been withdrawn.1
• A systematic review concluded that H2 antagonists were significantly more effective than placebo, bismuth salts were marginally superior to placebo, and antacids were not statistically significantly superior to placebo.2
• Alginate-antacid preparations appear to be more effective than antacids alone in the treatment of reflux oesophagitis, but less so than H2-antagonists or proton pump inhibitors, although they act more quickly.3,4
• Silicones have been shown to be effective in relieving gaseousness, but there is no clear evidence that they are more effective than antacids alone.5,6
REFERENCES